Healthcare Innovation
Healthcare AI Is Not a Technology Project
A model performing well in a study is not the same as an organisation being ready to deploy it safely. Healthcare AI is an operating-model change — and that gap is the board's to govern.
The most important question in healthcare AI is not whether the technology is becoming impressive.
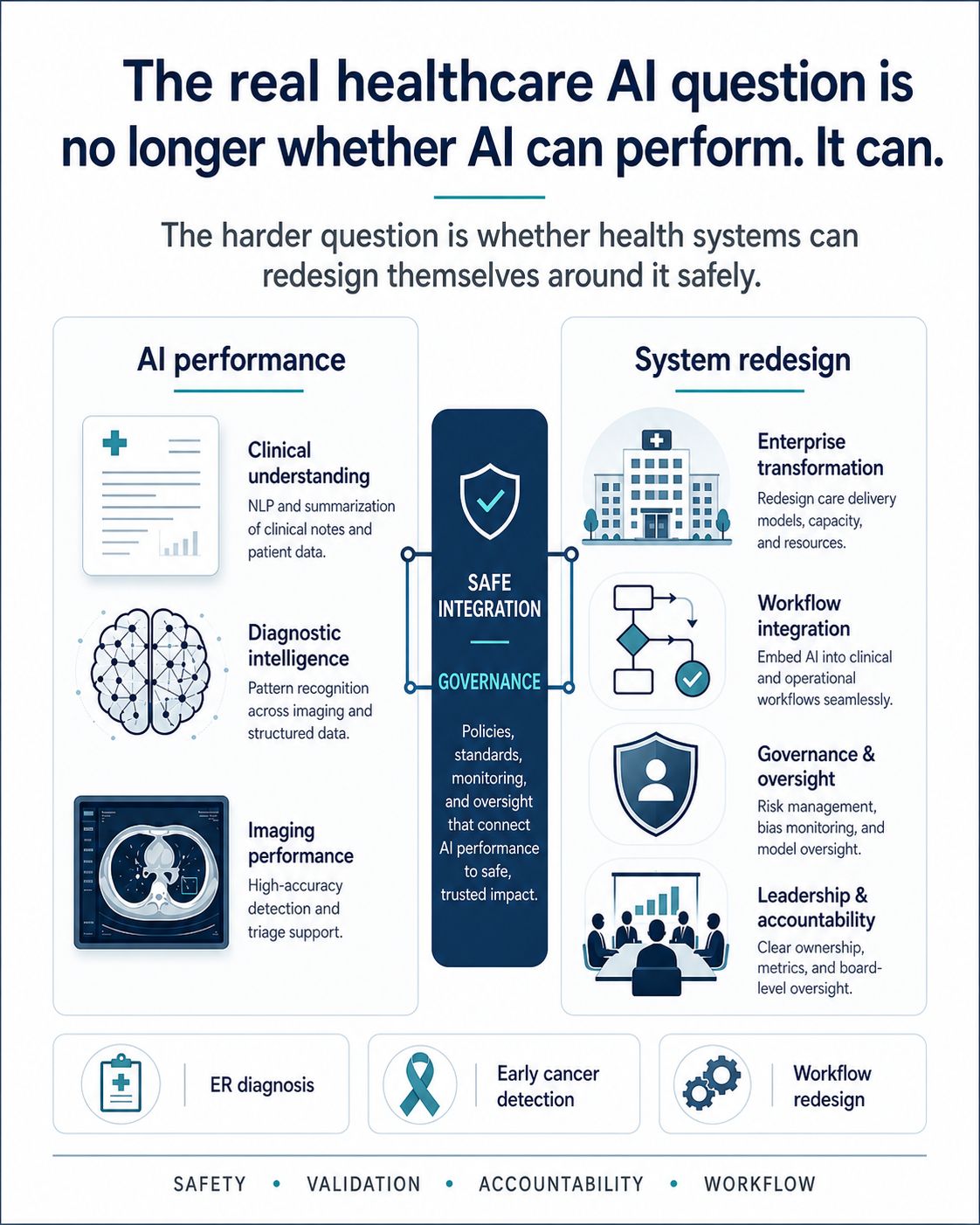
It clearly is. Recent studies and deployments show that AI systems are becoming increasingly capable in clinical reasoning, diagnostic support, image interpretation, triage and workflow automation. In some settings, the results are striking. AI systems can surface possibilities that clinicians may miss, process large volumes of information quickly and provide useful second opinions in high-pressure environments.
But a model performing well in a study is not the same as a healthcare organisation being ready to deploy it safely. That is the gap boards need to focus on.
Healthcare AI should not be treated as an IT procurement exercise. It is an operating model change. It affects workflow, decision rights, professional judgement, clinical accountability, patient trust, regulatory compliance and risk management.
Start with where the system sits, not which tool to buy
The first board question should not be: which AI tool should we buy? It should be: where exactly does this system sit in the clinical pathway?
Is it a second reader? A triage layer? A decision-support tool? A documentation assistant? A patient communication interface? A prioritisation engine? Each answer creates a different risk profile.
Authority: what happens when AI and clinician disagree
When AI and clinician disagree, what happens? Who sees the disagreement? Who decides? Is the override recorded? Is the outcome audited? Is the model improved as a result?
Without clarity here, the organisation is not governing AI. It is simply adding another source of ambiguity.
Accountability before scale, not after failure
If an AI-supported process leads to a missed diagnosis, delayed escalation or inappropriate recommendation, who is responsible? The clinician? The hospital? The vendor? The executive team? The board committee that approved deployment?
These questions are uncomfortable, but they need to be answered before scale-up, not after failure.
Evidence: benchmark performance is not real-world safety
Healthcare organisations should be cautious about extrapolating from benchmark performance to real-world safety. A system that performs well on written case data may not perform equally well in a messy clinical environment. It may not see the patient’s distress, hesitation, family context, physical appearance or changing condition. It may also perform differently across age, language, ethnicity, sex, comorbidity and socioeconomic groups.
That does not make the technology unusable. It makes local validation essential.
Trust is part of the infrastructure
Clinicians will not adopt systems they do not understand or trust. Patients will not accept systems they believe are being used to ration care or replace human judgement. Regulators will not tolerate black-box deployment without monitoring, accountability and evidence.
Trust is not a communications issue. It is part of the infrastructure.
The board’s job: from enthusiasm to disciplined implementation
The board’s role is therefore to move the conversation from enthusiasm to disciplined implementation. The agenda should include workflow design, clinical safety, data governance, model monitoring, liability, procurement standards, cyber risk, patient communication and measurable outcomes.
The prize is significant. Used well, AI could reduce administrative burden, improve access, support earlier diagnosis, help clinicians make better decisions and redesign parts of healthcare that are currently overwhelmed.
But healthcare does not need more disconnected pilots. It needs safe, governed workflow transformation.
The organisations that succeed will not be the ones with the most AI experiments. They will be the ones that can integrate AI into care pathways with evidence, accountability and trust.
Sources
- AI is starting to beat doctors at making correct diagnoses — Science, on a Harvard-led study of AI performance on text-based emergency cases and treatment planning.
- Mayo Clinic AI detects pancreatic cancer up to 3 years before diagnosis in landmark validation study — Mayo Clinic News Network.
- Executive Perspectives: AI-First Companies — Health Care Providers — Boston Consulting Group.
Distribution list
Be told when a new essay is published
Join the distribution list for occasional notes on governance, boards, AI, healthcare and growth capital. No marketing — just new essays.